Claire stared at the computer screen before cocking her head slightly to one side. She winced as a sharp pain angled its way through her neck and down her left arm. Her fingers went numb and then began to throb. Claire’s youthful good looks dissolved and she suddenly looked twenty years older. She stretched her arm and slowly began rubbing her neck to loosen the muscles. Her shoulders and neck had cramped up, making her whole upper body look tense and contorted. She reached for a glass of water and gulped down two more painkillers.
Why won’t this pain just stop? Why won’t these blasted painkillers work any more? They’re useless. I’m so sick and tired of this.
Three years previously Claire had been injured in a car crash and suffered two broken ribs, a fractured wrist and whiplash. Her ribs and wrist had healed completely within three months, but the after-effects of her whiplash refused to go away. The doctors were puzzled by her pain. Several scans had shown that her neck had completely healed, but the pain stubbornly remained. It was worse if she stayed in one place for too long. After twenty minutes, sharp jagged pains would arc up and down her neck. When she finally did move, she would feel stiff and achy all over.
Claire felt increasingly trapped and broken. Her doctor had prescribed several courses of physiotherapy without any long-term success. Now she was forced to continually take painkillers and anti-inflammatory drugs. They worked, more or less, but often left her feeling washed out and jaded. They were OK for stubborn ‘achiness’, but did nothing for the frequent sharp twinges of pain. Lately, her doctor had begun suggesting antide- pressants to lift her mood. Her response was always the same: ‘I’m not depressed,’ she’d snap. ‘I’m angry because that man who drove into me has taken my life away. I used to dance all night. Now I can barely walk!’
Experiences like Claire’s are not confined to injuries such as whiplash, but are common across a range of diseases. Conditions such as ‘bad back’, migraine, chronic fatigue syndrome and fibromyalgia can all cause pain long after the original injuries have healed or without any obvious cause that shows up on scans or tests. And even when there is a clear physical cause, as with illnesses like arthritis, heart disease or cancer, the pain often comes and goes without any apparent rhyme or reason. Doctors then feel forced to prescribe long-term courses of painkillers, but these can have side effects such as memory loss, lethargy and even addiction.
Claire and millions of others exist in a world of suffering; a place where even the simplest of tasks can amplify their pain. This often leads to anxiety, stress, depression and exhaustion, each of which serves to further enhance suffering in a downward spiral. Such vicious cycles are driven by newly discovered psychological forces that underlie the perception of pain. And crucially, this discovery offers a wholly new approach to the management of pain and illness that has the potential to transform suffering.
WHAT IS PAIN?
The commonsense view of pain is that it arises from damage to the body. This attitude was formalised in the seventeenth century by the French philosopher René Descartes with his ‘rope-pull’ model of pain: just as pulling a rope in a church steeple rings a bell, Descartes thought that damage to the body is a tug that causes the awareness of pain in the brain. For centuries after Descartes, doctors regarded pain in a similar light. The intensity of pain was thought to be directly proportional to the degree of damage to the body, which would mean that if different people had the same injury they would experience the same amount of pain. If no obvious physical cause was found, the patient would be regarded as malingering or making it up.
Since the 1960s, science has come to accept another model of pain known as the ‘Gate Theory’ developed by Ronald Melzack and Patrick Wall.1 They suggest that there are ‘gates’ in the brain and nervous system that, when open, allow you to experience pain. In a sense, the body sends a continuous low-level ‘chatter’ of pain signals to the brain, but it is only when the gates are opened that the signals reach your conscious mind. These gates can also close, which is what happens when your pain lessens or fades away. Opening and closing these pain gates is a phenomenally complex process. Although the details are still being worked out, it is clear that pain is far more subtle and complex than the traditional idea of damage signals being sent to the brain which are then passively felt. Pain is a sensation, which means that it is an interpretation made by the brain before it is consciously felt. To make this interpretation, the brain fuses together information from the mind as well as the body. In practice, this means that the thoughts and emotions flowing through your mind, both conscious and unconscious, have a dramatic effect on the intensity of your suffering. Not without reason did the ancient Greek philosophers consider pain to be an emotion.
PRIMARY AND SECONDARY SUFFERING
Suffering occurs on two levels. Firstly, there are the actual unpleasant sensations felt in the body – this is known as ‘Primary Suffering’. This can be seen as the ‘raw data’ that is sent to the brain from, say, an injury, an ongoing illness or changes to the nervous system itself (this is believed to lie, at least partly, behind such conditions as chronic pain syndrome and phantom limb syndrome). Overlaid on top of this is ‘Secondary Suffering’, which is made up of all the thoughts, feelings, emotions and memories associated with the pain. These might include anxiety, stress, worry, depression and feelings of hopelessness and exhaustion. The pain and distress that you actually feel is a fusion of both Primary and Secondary Suffering.
This insight is crucial because it reveals a path away from suffering. For if you can learn to tease apart the two flavours of suffering, you can greatly reduce – or even eliminate – your pain and distress. This is because Secondary Suffering tends to dissolve when you observe it with the mind’s compassionate eye. Mindfulness allows you to see the different elements of pain laid out in front of you. And when you see this vista, something remarkable begins to happen: your suffering gradually begins to subside and evaporate like the mist on a summer’s morning.
It’s important to understand that although the sensation of pain is created by the mind, your suffering is still real. You really do feel it. It exists and it can be genuinely overwhelming. But once you understand the underlying mechanisms of pain, you can begin to temper its power and the hold it has over you.
To go back to Claire, had she been asked to look inside herself a little more closely she would have realised that there was not one single ‘thing’ that she could label as an ‘ache’ or as a ‘pain’. Both were ‘bundles’ of different feelings that were constantly changing; becoming either more or less intense. There was the underlying unpleasant ‘tightness’ of the muscles and tendons in her neck, which were twisting her vertebrae slightly out of alignment and creating the most pronounced of her painful feelings. There were also twinges of outright pain – which felt like sharp spikes of electricity running through her muscles and down into her arm. And then there were patches of ‘numbness’ in her left arm and hand. These would alternate with pins and needles. Those were the obvious sensations of pain. This was her Primary Suffering.
But there were other feelings too – powerful emotions and disturbing thoughts that would frequently sweep across her mind, often with no apparent rhyme or reason. Stress, worry and exhaustion had become a way of life. Troubling thoughts constantly nagged at her soul: Why won’t this just stop? The doctors must have missed something, surely? Maybe I’m going to end up a cripple, or even dead. Are they too afraid to tell me? Such thoughts and emotions were constantly bubbling away in the background. And while they were often less obvious than the nagging feelings of pain, ultimately they were far more significant because they were central to the way that her mind interpreted and felt the raw feelings of pain. In a sense, they controlled the intensity or ‘volume’ of her pain. This was Secondary Suffering; and Claire had it in spades.
Claire’s Secondary Suffering had its roots in the five days she spent in hospital after her accident. They were the worst of her life. She was in considerable pain and on a morphine drip for the first twenty-four hours. She could cope with the physical pain – just. Far worse, however, were her turbulent emotions: her fears and worries for herself and the future. Neither she nor the doctors could predict the outcome of her neck injuries. Would she be partially paralysed? Would she be in pain for the rest of her life? There was also a sense of anger mixed with bitterness. The man who crashed into her didn’t appear to care. He just walked away from the accident with no cuts or bruises at all. He’d been drinking, but was just inside the legal drink–drive limit. Was he insured? It turned out he wasn’t. Every time she thought about it, Claire’s anger boiled over. Such thoughts and overwhelming emotions constantly washed across her mind. It was mental pain and just as real and tormenting as her physical injuries.
She lay in her hospital bed at night crying quietly to herself. She was wracked with fears and worries for the future, and ‘what ifs’ filled her mind. If only she had left home a minute or two later, then none of it would have happened. She’d had a feeling something was wrong before she had left home. Why hadn’t she waited just a few minutes longer?
After the accident and the subsequent months of physiotherapy, a new emotion was added to the list: depression. Claire refused to believe that she was depressed, but it was there none the less, gnawing away at her in the background. It wasn’t an all- consuming depression. It simply drained her of all energy and enthusiasm for life. Such powerful emotions as anxiety, fear, anger, worry and depression can feed into the mind’s perception of pain. Other feelings, too, can have an incredibly strong effect. Feeling tired and overwhelmed, fragile and broken, stressed and anxious, can all magnify suffering and tip you into a downward spiral. How often has the intensity of your suffering increased when you felt anxious, stressed, exhausted or sad? These emotions act like amplifiers in the mind’s pain circuits. They can open the floodgates of suffering.
The effect of such emotions can be observed with a brain scanner. Work at Oxford University,7 for example, shows the significant impact that even mild levels of anxiety can have on pain. Scientists at the university’s Department of Clinical Neurology induced low-level anxiety in a group of volunteers before burning the back of their left hand with a hot probe. As anxiety built, you could see the waves of emotion sweeping through the volunteers’ brains. This primed areas of the brain that collectively make up the ‘pain matrix’. It was almost as if the volunteers’ minds were turning up the volume on their pain amplifiers ready to ‘hear’ its first ‘notes’, so that they could take action to protect themselves. This meant that when the skin of the anxious volunteers was actually burned, they experienced far more pain and suffering than the ‘non-anxious’ volunteers. You could see this extra pain represented in the brain scans too. As the Oxford neuroscientists noted, anxiety primes the ‘behavioural responses that are adaptive to the worst possible outcome’. In other words, anxiety and other powerful ‘negative’ emotions prepare the body to sense pain quickly and with great intensity.
The reverse is also true. Reducing anxiety, stress, depression and exhaustion can lower the perception of pain and even eliminate it completely. This is one of the main routes by which mindfulness helps reduce suffering. Mindfulness soothes the mind’s perception of pain – essentially Secondary Suffering – by replacing it with a sense of peace and wholeness.
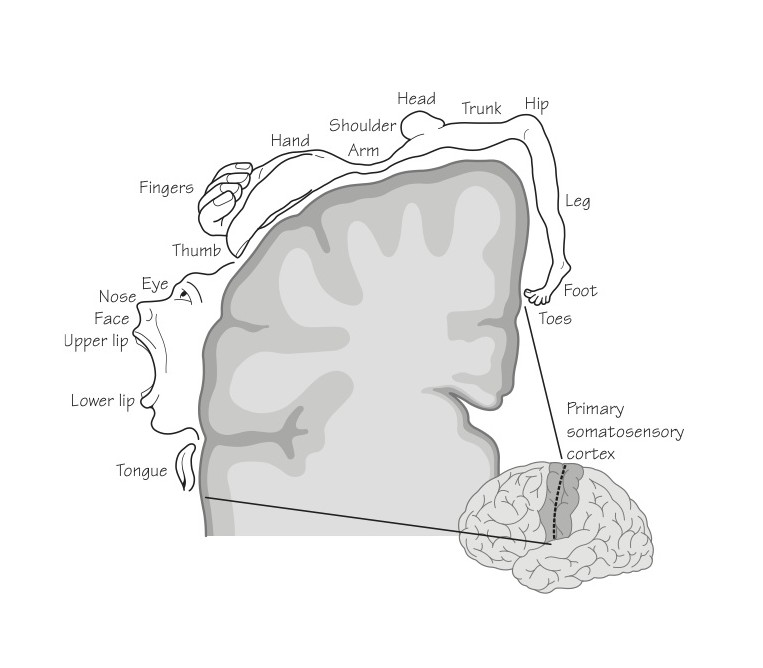
Neuroscientist Fadel Zeidan and his team at Wake Forest University School of Medicine in America decided to investigate this effect using scanners to map activity in different parts of the brain.8 They did this by exploiting a curious quirk of brain anatomy. Every part of the body is reflected in a specific part of the brain known as the primary somatosensory cortex. So if the sole of your left foot is brushed with a feather, an area of the primary somatosensory cortex lights up; if you feel a pain in your lower back, a different part becomes active. Neurosurgeon Wilder Penfield charted this brain region and produced a ‘map’ that reflects the human body overlaid on the brain (see illustration below). It was termed the cortical ‘homunculus’.
Fadel Zeidan and his team reasoned that if mindfulness affected the perception of pain, then this should be visibly reflected in the level of activity in the corresponding regions of the primary somatosensory cortex. To test this, Zeidan studied the perception of pain in a group of students. The students first had the back of their right calf burned with a piece of hot metal while their brain was scanned with the latest functional Magnetic Resonance Imaging (fMRI) scanner. Each was then asked to rate both the intensity and unpleasantness of the pain. If pain was music, ‘intensity’ would be the volume and ‘unpleasantness’ would be the level of emotion it aroused. As expected, when the students’ legs were burned the ‘right calf’ region of their primary somatosensory cortex lit up as the pain swept over them.
The students were then taught mindfulness meditation and the experiment was repeated. The results could not have been more different second time around. Activity in the ‘right calf’ region of the primary somatosensory cortex had diminished to such a degree that it had become undetectable. But not only that. Meditation increased activity in regions of the brain related to the processing of emotion and of cognitive control – areas where the sensations of pain are actually interpreted and ‘built’. These brain areas modulate the sensations of pain and give it ‘meaning’ before it is consciously felt. What’s more, experienced meditators (those who scored higher on a standard scale of mindfulness) tended to have enhanced activity in these regions and to experience less pain. That is, they tended to devote more brain power in this region to moderating the pain-related information – and to, in effect, turning down its ‘volume’.
Zeidan’s co-worker Dr Robert C. Coghill explains:
These areas all shape how the brain builds an experience of pain from nerve signals that are coming in from the body. Consistent with this function, the more that these areas were activated by meditation, the more that pain was reduced. One of the reasons that meditation may have been so effective in blocking pain was that it did not work at just one place in the brain, but instead reduced pain at multiple levels of processing.
And what of the students’ conscious experience of pain? On average they experienced a 40 per cent reduction in pain intensity and a 57 per cent lessening of pain ‘unpleasantness’. Perhaps the most surprising thing was the amount of practice required to achieve this level of pain relief: just four training sessions of twenty minutes each. Remarkable though these results were, they masked something even more intriguing. The more accomplished meditators suffered far less than these averages might suggest. They experienced a reduction in pain intensity of 70 per cent and its unpleasantness was reduced by 93 per cent. This meant that it could barely be felt and hardly bothered them at all. Overall, said Zeidan, mindfulness produced a greater reduction in pain than standard doses of morphine and other pain-relieving drugs.
Loosening the bonds of pain
Secondary Suffering can be seen as resistance to pain. It is entirely natural to struggle against and resist pain with all of your might. You want to eliminate it. Stamp on it. Do anything at all to get rid of it. This is absolutely understandable. But what if this was also precisely the wrong approach? What if, in your bid to eliminate pain, you were actually creating far more of it instead? This is the lesson from Zeidan’s research and from many other studies too. And this holds true not just for pain, but for many other disease symptoms as well. Stress, exhaustion and depression can all be made far worse through resistance.
But if the act of resisting pain can make it worse, the converse is also true. Acceptance of your pain can actually diminish it – and might even get rid of it completely. Allow us to explain this seemingly outrageous idea. Neuroscientists have a saying: ‘What we resist persists.’ In other words, if you resist the messages that your mind and body are sending you, those messages will keep on being dispatched (and felt) until you accept them. This holds true not only for messages of pain, but also for thoughts, feelings, emotions, memories and judgements. If you mindfully accept (or feel) these messages, they will have done their job and will tend to melt away of their own accord.
Mindfulness meditation creates a sense of safety, of space, in which you can begin to tentatively explore the raw sensations of pain and, as such, it is the vehicle through which you can begin to accept these messages. And when you do so, you will often find that pain waxes and wanes quite dramatically. There can be long moments of normality followed by flickers or spikes of pain. There are often different sensations too. Some are hot. Others cold. Some feel ‘tight’, others throb, while still others feel sharp or stabbing. Not all are completely unpleasant. The different sensations often rise and fall like the waves on the sea. They constantly change in character and intensity. By exploring each of these different sensations, moment by moment, you come to accept that they are like black clouds in the sky: you can watch as the sensations arise, drift past and disappear again. Your mind is like the sky and individual thoughts, feelings, emotions and sensations are like different types of cloud. So in a sense, mindfulness teaches you to observe the weather without becoming embroiled in it. And no matter what happens, the sky – your mind – remains untouched by it.
It is important to realise that mindful acceptance is not resignation to your fate. It is not the acceptance of the unacceptable. It is simply the acceptance of the situation as it is, for now, at least. It is a period of allowing, of letting be, of non-resistance, so that you cease to struggle. And when this struggle ceases, a sense of peace takes its place. Secondary Suffering then progressively diminishes. Often as not, Primary Suffering will begin to do so too.
We can explain this to you in minute detail. We can cite numerous scientific trials that prove the point. We could even show you scans of your own brain as it ‘builds’ the sensations of pain from all of your thoughts, feelings and emotions – but only when you have experienced the power of mindfulness for yourself will you truly believe it.
This is why it is called a practice. Accepting pain can be difficult. It’s just better than the alternative, which is to live in a state of perpetual suffering.
Countless participants on our Breathworks courses have discovered this for themselves. Claire was one. She found that when her neck began to hurt she was also assailed by fear, anger, stress, sorrow, hopelessness, despair and exhaustion. So not only did she feel the initial unpleasant sensations in her neck, but she was also swamped with yet more suffering. It was almost as if she was struck with an arrow, and when she reacted to it she was then hit by a second one. Now she had to bear the pain of two arrows – that from the second being caused by resistance to the first. It is an entirely natural response. In fact, in cases of acute, rather than chronic, pain, it might even be the best response because it’s a powerful driving force to take yourself out of danger. When it comes to chronic pain and illness, however, it is often precisely the wrong solution because it simply compounds your suffering. And, of course, it can then seem as if you’re pierced not by two arrows, but by many, many more.
Accepting the sensations of Primary Suffering allows the Secondary Suffering to take care of itself – and to progressively diminish. Claire discovered that she could resist pain for days or even weeks. She could distract herself with alcohol, cigarettes and food. She could squash the pain with powerful drugs. If those failed, she could ignore the pain – for a while, at least. But all this came at a cost: the rest of her life. She discovered that in ignoring and walling off the pain she had also isolated herself from all that is wonderful and precious about life. The world became increasingly wan and grey. Food lost its flavour and texture. She no longer laughed or cried. Her love life declined into irrelevance. All this meant that when she could no longer maintain the struggle, she simply crashed and burned. So not only did the pain return, but, with all of the things that normally sustained her love of life having evaporated, she was left feeling fragile and broken. No wonder her doctor wanted to prescribe her antidepressants.
After three years of struggling, Claire embraced mindfulness – not because she believed that it would work, but because she was desperate. And when she began to mindfully explore the sensations of pain, something remarkable and counter-intuitive began to happen. Not only did the pain begin to subside, but she began to experience all of the good things that had been squeezed out of her life too. It opened the door to a wealth of emotions such as happiness, love, compassion and empathy, as well as sadness. Claire realised that life is bittersweet, and when she let go of expecting it to be either wholly wonderful or truly distressing and to hold in an honest heart a delicate mixture of the two, she felt increasingly relaxed and open. Through facing up to and becoming sensitive to her own predicament, she became a happier and more centred person with greater empathy for others. She also began to heal.
Taken from our new book Mindfulness for Health: A Practical Guide to Relieving Pain, Reducing Stress and Restoring Wellbeing by Dr Danny Penman and Vidyamala Burch
Buy from Amazon UK
Buy now from Amazon US (Sold as You are Not Your Pain)
‘A beautiful and compassionate book, Mindfulness for Health will put you back in touch with the extraordinary person you already are’ Professor Mark Williams, University of Oxford
‘This book provides an extremely effective and elegant mind-body approach to healing . . . Highly recommended’ Jon Kabat-Zinn, PhD, author of Full Catastrophe Living and Coming to Our Senses
‘In a world of much suffering this book is a gift of wisdom and practical help’ Professor Paul Gilbert, PhD, OBE, author of The Compassionate Mind
References
1. Wall, Patrick D. & Ronald Melzack, The Challenge of Pain (Penguin Books, 1982), p. 98; Melzack, R. Wall, p. D. (1965), ‘Pain Mechan- isms: a new theory, Science, 150(3699), pp. 371–9.
2. Cole, Frances, Macdonald, Helen, Carus, Catherine & Howden-Leach, Hazel, Overcoming Chronic Pain (Constable & Robinson, 2005), p. 37; Bond, M., Simpson, K., Pain: Its Nature and Treatment (Elsevier, 2006), p. 16, offers an alternative definition from the International Association for the Study of Pain as acute pain (lasting less than one month), sub-acute pain (lasting one to six months) and chronic pain (lasting six months or more).
3. ‘Health Survey for England 2011’, Health, social care and lifestyles, Chapter 9 Chronic Pain, The Health and Social Care Information Centre (NHS) 20 December 2012, www.ic.nhs.uk/catalogue/PUB09300.
4. Gaskin, Darrell J. & Richard, Patrick (2012), ‘The Economic Costs of Pain in the United States’, Journal of Pain, 13(8), p. 715.
5. ‘Health Survey for England 2011’, Health, social care and lifestyles, Chapter 9 Chronic Pain, The Health and Social Care Information Centre (NHS) 20 December 2012, www.ic.nhs.uk/catalogue/PUB09300.
6. NOP Pain Survey (2005), 23–25 September, on behalf of the British Pain Society.
7. Ploghaus, Alexander, Narain, Charvy, Beckmann, Christian F., Clare, Stuart, Bantick, Susanna, Wise, Richard, Matthews, Paul M., Nicholas, J., Rawlins, P. & Tracey, Irene (2001), ‘Exacerbation of Pain by Anxiety Is Associated with Activity in a Hippocampal Network’, Journal of Neuroscience, 21(24), pp. 9896–903.
8. Zeidan, Fadel, Martucci, Katherine T., Kraft, Robert A., Gordon, Nakia S., McHaffie, John G. & Coghill, Robert C. (2011), ‘Brain Mechanisms Supporting the Modulation of Pain by Mindfulness Meditation’, Journal of Neuroscience, 31(14), pp. 5540–48. See also the accompanying comments regarding morphine effectiveness by Fadel Zeidan of the Wake Forest University School of Medicine at http://ow.ly/i8rZs.





